My search for grace and meaning after a former care partnering life with a wife who suffered from Parkinson's disease and dementia giving her a confused and disorienting world.
Cheryl’s Parkinson’s disease interlaced with dementia has taken a turn to the negative over the past three months. It is tough but necessary for us to explore extra help and other options to our living situation.
I feel a sense of sadness. It is not exactly that I have failed because I recognize in my heart that her disease has a progression. I suppose it is a progression that I had not anticipated.
I also feel a sense of relief, an acceptance of the fact that I cannot do it all alone anymore. I recognize that we have to do something different. That first recognition came when I decided to buy a new bed and change our sleeping arrangements. At least, I thought a split king would keep us from awakening each other at night.
We drifted off to bed about 10 PM after watching a couple of her favorite shows on television and visiting with her sister for a couple hours. We probably eventually fell asleep about 10:30. Overnight I got up to go to the toilet twice and the second time around 3 AM she got up with me and seemed as though she wanted to stay up. I had prepared to sleep on the sofa bed we had and then she came out looking for me. We had our often discussion about church and I suggested we lay down for two more hours and then get up. She got up at quarter til noon.
I got up around 8:30. It was bliss.
I took the time to call the assisted living facility nearby that had housed both of our mothers at the end of their life. I still refuse to believe that we are here yet BUT it does not hurt to find out about various options to move forward from here.
I also set up a couple doctor appointments. She is having problems hearing occasionally. And I wonder about a UTI.
It is a tough decision to make. It seems to me that I might not be able to provide the care that Cheryl needs overnight. It breaks my heart to admit it.
Care giving to your spouse opens a whole new line of thought about being of service to others. Throughout my life I have sought jobs that both interested me and allowed me to be of service to my employer and their customers. Sometimes to financial detriment of the guy paying my salary. Good customer service extends to all other areas of life.
These days much of my time is spent in caring for Cheryl. She has taught me new methods of coping with the current situation. This is especially true as the dementia aspect of her Parkinson’s disease seems to take over from a mere (if there is such a thing) movement disorder to a degeneration of her cognitive ability. Simple sleep seems to help.
These days sleep does not always help. Her mind is constantly confused. In any single conversation she can be old and young, a student ready to go to school, our children might live here with their children and I might be someone else.
Oftentimes my immediate reaction to unsolicited advice is to ignore it because I assume that the advisor has their heart in the right place. Pushy people can insist that I’m doing it wrong but it is possible to listen past this and hunt for the useful nuggets of information.
Today Jane apologized for jumping up to find Cheryl a different cup to put her soft drink into at the pizza store last Tuesday. It was both unsolicited and surprising. I ignored it and when she came back with a coffee mug I poured part of Cheryl’s drink into it. It was a good solution and Jane’s apology and later her admonishment when I said that it was unnecessary reminded me that I am not the only solver of problems. Jane’s background is special education with kids that have special needs and although Cheryl is not on of those, some of the same rules apply.
For quite some time now I have been merely moving Cheryl’s giant plastic glass of soft drink away from any gyrations that occur with her hands as she engages in conversation. It never occurred to me to merely request a smaller additional glass to put her coke in. Something that was easier to deal with. AHA (dammit I missed that one.)
FIND RESPITE – If you’re focusing most – if not all – of your time, energy, and resources on caring for a loved one with dementia, you may find you cannot sustain doing so over the long-term. With proper self-care, you can relax and recharge, manage caregiver stress, and become a better and more effective caregiver. Consider sitting on the porch and reading a book, a brisk walk, a cup of Starbucks, an ice cream cone, a massage, a warm bath with soothing scents. These things need to be done regularly in order to maintain your own health.
I read these words again this morning. Only I can find respite for myself. That is often hard for the care person to see clearly. I went outside to straighten the small garden area we have. The steady rain over the past few days which has darkened Cheryl’s mood also has loosened to soil around a Jacob’s hook holding a hanging plant Cheryl got for mother’s day.
It occurs to me this morning after another overnight of strange behavior that discussing her actions overnight has no useful purpose. So, I have not this morning. I will wait and see if I need to discuss it with someone else.
Part of Carpe Diem is to stay in the present. The past is the past and while it gives me a hint as to what is coming, it is a very dim view with poor illumination.
In a past episode of “Ghosts” the young woman protagonist uses the term “maybe” instead of a direct “no.” Cheryl says, “I’ll think about it.” Reading the care giver’s guide to the galaxy book which is a part of the class I am attending to learn some things the communications chapter discusses saying “no.” It talks about the implications of negativity which go along with saying no. I have noticed that most times people cannot say no with out offering some explanation to lessen the blow of the no.
It is much harder with a dementia patient. The no may be a greater blow than one can imagine. But sometimes it is very important to the care partner to express “NO” and then explain the the care receiver why no is important this time and then discuss alternatives that may sound like “we’ll see.”
So what can the Care Partner of The Year 2021 do with all of this wonderful knowledge? In an inadvertent fluke of fate and its fickle finger Patty send me an email with the information about a Caregiver’s Class put on by Catholic Charities of Southwestern Ohio. I am all for being as educated as I can about how to take care of Cheryl better by taking care of myself.
Being an engineer and amateur scientist I thirst for knowledge. That is corny but true. The problem with that statement overall is that there is no complete solution to Parkinson’s with dementia added. There is not even a partial solution. Cheryl’s sister hopes for a cure. I do not hold that same hope. That being said, the situation is not hopeless.
I bought a book called “Dementia Reimagined”. I was hoping for a cookbook style answer manual. It was not that at all. It is an incredibly tiring tome about public policy and where it fell into the dumper over the years. Engineers are always hoping for a cookbook for their situation. When this happens, do this. Alas there is no such manual for life situations as defeating as PD with dementia.
But back to the help-book, It seems as though many of the ideas I have discovered on my own or others have told me about I merely have been ignoring them. Early in the book it talks about developing goals and achieving them. These are not care-giving goals. These are goals that allow the care-giver some relief.
Initial focus is on setting a goal or several goals and development of a plan to achieve it or them. The goals discussed are relaxing activities for the care giver. So, it is something you want to do. It is also something that is reachable and realistic. Something you can accomplish in the near term.
What do you want to do?
How much of it do you want to do? (more specifics)
When do you want to do it? (timing helps to plan)
How often do you want to do it? (repetitive relaxing activity)
This same technique can be used to plan any sort of activity, of course, but the book’s focus is care partnering and care partner health. Additionally this portion of the text asks the maker of promises and planning to predict the probability of achieving your activity. There’s an implied deep need here. Something that you may really feel like you want to do but have little chance of achieving. A life lesson in the manner of understanding that not all wants are achievable. (How driven are you to get to your goals)
The next portion of the focuses effective communication and recognizing emotional and stressful situations. Two forms of communication discussed are assertive and aikido. A comparison of these styles of communication is Assertive:”stand tall” vs. Aikido:”standing with” This portion of the book takes me back to my educational psychology classes and discussions about defusing confrontational situations.
ASSERTIVE
setting limits
asking for help
advocating for another
making difficult decisions
dealing with difficult styles of communication
AIKIDO
defuse emotional situations
help others feel understood
reduce anger
balance emotions to allow dealing with others
As I go through the rest of the book I will report anything else of interest to me.
Scott was here last night to be with Cheryl while I visited my stock club meeting. The fourth Monday of every month is the meeting of our little stock club. We started this little club in 1984. Over time we swelled to 20 members but the past few years attrition and death has shrunk our number to eight. And over the past few years the meetings are more social than business. Where else can eight old men get together and trade war stories about getting old, fortunes missed, grand children achievements, the proper temperature of beer for drinking, Parkinson’s disease, prostate problems, cataracts and hearing issues, but in the backroom of a local watering hole near a railroad track? It is always fun and over the years I have rarely missed it.
Before I left for the meeting Cheryl’s stomach was bugging her a bit as happens occasionally after her 4 pm meds. When I returned I asked her if she had eaten anything. She said yes but behind her Scott shook his head no. She answered my question how she thought I wanted her to answer it.
Eventually about 11:20 pm we went to bed. Over night she was fidgety and got up at 2:30 a.m. to make a list so she would not forget something. I sat her at the kitchen table with subdued lighting and with paper and pencil she worked on her list.
Her list is a business memory. I sat with her and about 3 a.m. she decided to sleep some more and finish later on. Buzzing around in her mind these days is the thought of creating a database of birthdays for the people in her family. Many times and in many instances she has started this task. Just like engineers this thinking starts with a pad and paper. Often sketches are made to indicate data flow and information input. Just like an engineer Cheryl’s notes switch back and forth from cursive to printing. And although she had an urgency about this activity in the very early morning hours, she had no ideas about what it was or what it was for in the daylight hours.
She seems so fragile to me in the morning lately. She is still working on the remnants of some dream as she awakens. This morning she got up and went into the bathroom. I got up also and put clothes on, got some coffee for myself and turned on the CBS news to see if any new wars developed or any movie stars got divorced overnight. About 20 minutes later I went back to check and see if any help was needed or if there were any special breakfast requests. She was seated on the closed toilet waiting for someone to bring more toilet paper. I showed her where the extra rolls were and asked if she wanted cereal for breakfast. Yes was her reply. I returned to the living area.
About ten minutes later I went to check again and she told me she was still waiting for someone to bring toilet paper. The thirty minutes of database design time in the middle of the night messed up her waking pattern.
More and more she seems to have a slow switch from early morning confusion to present. I have not found a solution to any of this confusion and delusion. I listen to her conversation and make a lot of rapid decisions about how to respond. If it seems like she is getting ramped up about someone coming (that I know is not) I try to gently steer her toward the correct thinking. If she is getting fired up about having a family gathering I merely agree with her plans.
On this particular morning she was concerned about whether David was going to show up any minute to cook the Thanksgiving turkey. It took several repeated conversations about date and time but eventually she seemed okay that Thanksgiving day was not today. Over several hours she came to the conclusion that she should take a shower and get ready for her exercise class. Over those same several hours I planted various seeds of the idea about taking a shower and looking for exercise clothes to wear.
Me and how I feel – It is wearying for the care partner to both console and encourage and direct and deflect her delusions and my own background anger (too strong a word – disappointment?; discouragement?; vexation?) with her brain and how it is operating with PD. My question – Why can’t she have the movement issues without the mental disability? (God are you listening? Why her? She has always been a sweet person. Why did you dump this crap on her?)
Observations about my reaction to her needs – (Shit! Not again. This is the same conversation we had 15 minutes ago. whiskey tango foxtrot.) How can I help dear? Cheryl – you can’t help. Perhaps not but let me hold your purse for you while you get out of the car.
Is this genuine love? … To have and to hold from this day forward, for better or for worse… Those where part of the original agreement. Too late to back out now. She looks so sad and distraught when she realizes that she needs me to help her up from the chair because her scoocher is busted. It is heartbreaking.
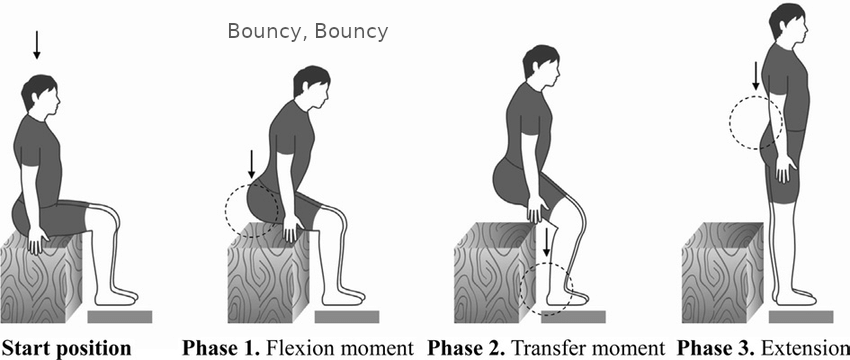
When trying to get her scoocher going to get out of the chair, off of the sofa, out of the car, out of the booth at the restaurant, Cheryl bounces. My younger sister coined this term to me when she said that after spending so much time in a hospital bed with a variety of blood cancer, her scoocher no longer worked. It was hard for her to get into a wheelchair, into the car, out of the car, and so on. Laura is no longer of this earthly existence. Cheryl’s scoocher still works sort of. She scooches to the edge of a chair and grabs, pulls or pushes herself up. As many as six different PT instructors and her doctor and NP cannot get her to understand bending forward to stand, so she bounces and pushes.
Actually this guy in the picture sums it up pretty well. Since he did not lean forward enough to get his head over his knees, his center of gravity is behind his ankles. If he has really massive toes and strong glutes it will work. At step two Cheryl does the bouncy thing to get momentum to throw herself up.
To a parkie who is constantly worried about falling on her face, it is understandable to avoid leaning forward too far. Her solution is to lean away from the direction she is going toward. Sometimes she falls backwards.