My search for grace and meaning after a former care partnering life with a wife who suffered from Parkinson's disease and dementia giving her a confused and disorienting world.
It started like a normal morning I got up at 7:30 or so and left Cheryl sleeping soundly in bed. I put the last of yesterday’s coffee in a mug and told the microwave one minute. I woke up the Wordle on my tablet and went out to get the paper. Someone, perhaps our new neighbor brought them inside the front door. I picked up Jeanne’s paper and her mail. She is 98 and does not go out much or downstairs much. I carried her stuff up to the bag she hangs on her door for that purpose. I noted that she had not retrieved yesterday’s paper from her bag. (Maybe I will check on her later.)
I watched the news on hurry up speed up as I had prerecorded it when it came on at 7 AM. There is still a lot of things going on that I have no control over. But at our little group of condos, the decks are fixed, the roofs are on and the trim is newly painted. The landscape folks want me to accept the quote for scraping snow and putting out ice melter. Winter is coming.
I started thinking about Cheryl, winter, gloomy weather, sundown syndrome and care partner stuff. About 9:30 AM I went to see if she was awake and ready for breakfast.
I found her in that in between sleep and wakefulness that we all experience in the morning. Usually my right hip tells me (You are old buddy boy. Move your ass.) to get up and move around. Cheryl and I exchange small talk and teasing for a bit.
“Do you want a kiss on your ear?”, I say.
“No”, she replies.
“What about on this cheek?”
“Okay.”
“Scrambled eggs for breakfast?”
“Sure.”
“Toast with grape jelly?”
“Yes.”
“Want any bacon?”
“Not today.”
“I am going to get your rollie chair. I will be back.”
She is more comfortable these days with me scooting her out of bed and into a transfer chair. We go into the bathroom for a trip to the toilet, pills and then into the kitchen for breakfast.
On this day when I sat her on the toilet she began to shake, sweat and cry a little. “My arms really hurt.”, she said. She initially complained about the toilet seat being cold. I ignored that because she often makes that complaint. Her hands and arms were shaking violently and I held the glass and straw for her to take the meds that I placed in her mouth one by one. We have done this before but not with the shaking action.
I had been gently rubbing her left arm as I helped her take her pills and she asked me to stop. She told me her arms were hurting. I got her a nsaid pain reliever that had been prescribed by her doctor for occasional pain occurrences.
It is a little chilly in Ohio this morning and although our thermostat reads 75 F in the bathroom it seems even to me a little chilly. In the middle of moving her from the toilet to the transfer chair, I got her heavy fluffy ugly pink bathrobe on her. I combed her hair and rolled her to the kitchen.
Apple juice, scrambled eggs and jelly toast later, the shaking and sweating were gone. Her arms did not hurt anymore. She still reports a little pins and needles tingling in her hands and fingers. The meds seem to be working but this whole episode was new. It began after I had gotten her out of bed with no complaint and onto the toilet, also with no complaint.
A cold toilet seat seemed to start everything. And that is very weird. Maybe I need a couple of these snazzy covers.
This week for lack of a better description was doctors’ week. We saw both our personal care physician and Cheryl’s neurologist a movement disorders specialist. He made some minor adjustments in her meds schedule and added one new one to help with anxiety and perhaps some depression he detected by interviewing Cheryl.
Prior to these visits over the past couple days Cheryl slept poorly. This morning she is sleeping in. She was relieved last night when I helped to bed with the fact that we had nowhere to go today. We had no doctor visits. She did not have to be on her toes to answer questions about how she feels that could make her feel sad. I think she is very aware that she can cry easily and is unable to control that response. Her neurologist is very gentle and recognizes her disease’s progression in her body.
It was very hard to maintain her showtime persona yesterday and the day before. I am gladdened by the fact that it is over for a few months.
I helped her up out of bed and into the kitchen for breakfast but I was premature. She kept her eyes closed in the kitchen. She seemed uninterested in breakfast after all. I asked her if she wanted to sit in the lounge chair and doze for a bit. She did.
I talked to the physical therapy folk to schedule the PT recommended by her neurologist. Eventually she awakened as I put a pillow under her left side because she was drooping that way in the lounger.
I rolled her back to breakfast. She ate and looked at the paper. She did not work the puzzles.
I talked to my Portland sister. She often makes me rethink things. The doctor has diagnosed Cheryl with some mild anxiety and perhaps depression. The brain floats in a sea of proteins and chemicals. Parkinson messes with that. I do not always recognize my own needs as a care partner.
In my never ending battle to keep us safe and healthy and because Cheryl kept pressing me to do it, I scheduled us for a second booster shoot for the covid virus yesterday.
I got some chicken out of the freezer for dinner and helped her get moving in the morning. The morning was busy for me because it was my last care partner class. From that I have a mountain of valuable information about various service providers for the future. We are not there yet but in a few years we will be.
Linda appeared a little early and we chatted for a bit and then I was off to class. When I returned Cheryl had gotten cleaned up and dressed herself. I think the big new bed is giving us better rest overnight.
Our appointments at Walgreens were scheduled for 4 PM and 4:10 PM. We got to the store with plenty of time to fill out forms and prove who we are. Except for me. I had forgotten my wallet and ID. (Alas and drat!) As Cheryl came down the aisle pushing her U-Step walker I explained that I had forgotten my wallet. I asked her to sit down near the pharmacy desk and I would return in a few minutes. This Walgreens is about 5 minutes from our house. I zipped home and back to the store. When I returned she was sitting in the chair filling out a form on the clip board that the pharmacy assistant had given to her. Ordinarily this small task would have been confusing and incomprehensible to her. She had even found her ID and previous covid info in the purse of many pockets. I am beginning to understand that much of her confusion and mental fog of late may merely be poor sleeping patterns.
It is hard to overemphasize how important good sleep and rest is. The big new bed seems to help. One less Carbdopa/Levadopa CR seems to be beneficial also. She seems brighter during the day and not so inclined to pund around in her office at night. She is sitting in her recliner with me to watch a show or read a magazine article more during the past couple weeks.
She had plenty to eat at dinner. She even complained that I had not made gravy to go with the chicken. It was a normal (mostly) conversation during dinner between two people who had been married for 53 years. (Smiley face here) Later in the evening she felt a little chilled. I went to recover her sweater from the backseat of the car where it had been warming in the 90 degree heat for several days. We sat for a bit longer and then she got ready for bed. She returned and we watched the PBS show NOVA for an hour and we went to bed at 11 PM.
We were up again at 1 AM until about 3 AM. I am going to blame the booster shot. I was having difficulty also.
Today we slept until after 9 am. She seems rested. I know I am. It is off to the doctor today for our semi-annual wellness check. I feel well. She seems well.
Last night was the first dose of donepezil which may help with Cheryl’s confusion and dementia issues. It has two main side benefits (effects) in addition to the myriad of others that seem related to any drug regimen. The side effect I am most concerned with is insomnia. I will be watching for this closely over the next few nights as her body adapts to the medication. The drug literature suggests a two week or so adaptation period. I am hopeful today.
The dose in this series of pills is 5 mg. The intent is to discover the patient’s tolerance for it. The dose will be increased over time. If one eats a little bit of peanut butter each day when one is little, one will not develop an allergic reaction to peanuts. If you eat a little bit of dirt each day as a child you will develop a tolerance for a lot of things later in life but your parents will go through a really annoying diaper period.
Nevertheless last night was peaceful. One trip to the waterproof room and no extra laundry in the morning. Seven AM meds consumed on schedule. Breakfast of yogurt and Pillsbury refrigerator rolls rounded out the morning.
Exiting “news” today from the world’s largest advertising company Meta formerly know as Facebook, new tools are available for Instagram whatever that may be. (I am old.) All the major stock market indexes plunged (not fell) into bear market territory. The Fed is wondering out loud about where to set interest rates. Nervous investors are placing their bets. Bitcoin aficionados are moving their money so quickly the major exchange called a halt. (Think of all those computers mining bitcoin settling into stasis.) Ho hum. And it is going to be hot today on the east coast where all the news comes from. Stay hydrated!
Another day begins. Cheryl seems to be moving well. She can try out our new grab bar that was installed yesterday on the wall near the shower to help with getting in and out of the shower. I have no control over the things that CBS has decided is news today, so, although I am mildly interested, I do not spend much time on it. Cheryl is quietly watching the news after eating her Pillsbury refrigerator rolls and yogurt with OJ.
The Wordle today was easy. I got it on the first guess. Today life is good.
A mild mannered drug used to treat confusion in patients with dementia. Often the only chemical of consequence for treatment of Alzheimer’s disease. A little humor there. The previous choice was rivastigmine which Cheryl could not tolerate.
We’ll see. I am fearful of giving her some thing else that is going to make her feel like crap all day long. The slow movement and mental confusion is somewhat easier to help her with than persistent nausea. Rivastigmine did that to her.
We are starting this drug on the thirteenth of the month. That cannot be good.
beliefs of simple things, such as, whose job is it to do this chore or that chore. Mowing the lawn, for example, is it a male or a female job? And why do most people grow grass around their property that is not native to their part of the continent? From my perspective it is a male chore to mow the lawn.
As a boy – it was mine
How do things like this get started? I have always – at least in my memory – thought of mowing the lawn as a man’s job, chore, duty. No doubt dating to my childhood when it was the chore I was assigned somewhere around the time my brother graduated high school and left for the Massachusetts Institute of Technology. I would have been about twelve years and certainly tall enough to push a lawn mower and not injure myself. I have no memory of whom in our family mowed the weeds before me. I assume it was my older brother but I have no memory of watching him do that task but he probably did. He is gone now and I cannot ask him.
It was my chore to keep the estate spiffy and shipshape. Did I like it? Indeed I did not.
As a man – I thought mine
Over time things get ingrained, ground in, always assumed. That is your job. Just do it. When we bought our first house I purchased or somehow obtained a ultra low end lawn mower. It was a tiny back yard and much was given up to english ivy. Why I ever decided to remove much of the ivy and turn it into lawn is beyond me now but at the time we had one child with another on the way so a place for the kids to play was probably the motivation. I also built some garden boxes, a sand box for the little people to play in and the neighborhood cats to crap in, a raised vegetable garden area, a strawberry bed, a swell picnic table and a rabbit hutch with rabbits. It was a busy six summers there. I was not yet thirty years old. We were fertile. We had three children when we moved to the big house.
I had my own schedule when it came to maintenance items such as mowing the lawn. Building the lawn is way more interesting and fun than mowing it. Occasionally she and I would argue until I discovered that she actually enjoyed mowing the lawn. She would mow it and I would assume incorrectly that she was trying to show me up. Our first lawn was tiny and I had an electric mower with a 100 foot long cord. She loved it and she could do it during nap time. It was quiet. I gave up the maintenance duty on the lawn.
As a father – my son’s job
When we moved to the new big house with the new big lawn and the mostly dead American elm in the back I bought another 100 foot long extension cord. This worked for awhile until it became too cumbersome and I gave in to purchase a low end gas powered mower from a big box store.
The elm was removed, another vegetable garden was installed and a cherry tree added to round out the crop yield. The kids were growing rapidly. She and I decided that it would be good for the kids to have some responsibilities around the homestead and its maintenance. Some jobs more important than making sure that the two freezers did not contain too much food. We gave our middle son the duty of mowing the lawn and he seemed to like it initially. I eventually gave in and bought a riding mower and he liked it even more. There are many fine stories to go with the riding lawnmower of questionable manufacture.
Household chores in our new life with PD
In our current life with this disease of Parkinson we try to avoid having it be the center of our life and rule over all that we do but some days that just seems impossible. Some days the distraction is insurmountable but over time we have come to grips with the fact that it is simply more efficient for me, the husband, the father, the care partner to assume most of the regular chores and Cheryl can do ones that she deems need doing and she is up to the task that particular day. Some days she does nothing other than survive. Some days she busies up her day with several little things which takes a toll on her physical well being and the following day is a survival day. I like routine so I have selected certain days for certain major chores.
I have developed three laundry group days. Monday is wash-the-bed-sheets day. Wednesday is wash-the-towels day. Friday is wash-the-clothes day. On Friday I split the wash into loads that make sense to me not her and we have sparred a bit about what is in each load but we do not any longer. I believe she has lost interest in laundry and its routine. On wash-the-clothes day I also look at the checking account to be assured that we are not getting too rich and do any book keeping and bill paying. Over time I have put many regular expenses on automatic.
On a daily basis there are a myriad of other little things that I do to keep things rolling along. It now seems trivial when I reminisce about my anger with her stealing my thunder and mowing the lawn without telling me. (Yes, that was the source of my once ill-placed anger.) These days I look forward to being with her and caring for her.
Morning routine includes dressing the bed. In our other younger life I never did this. In this life I have made some adjustments to suit me since it is principally my daily job. Evening routine includes making dinner and when I am out of gas or merely think we are isolating ourselves too much we go to a restaurant and let them make dinner.
Cheryl has had difficulty lately with an evening routine that allows her to wind down and sleep through the night. We have been adjusting the timing of her evening meds. Because she often complains of taking so many pills, we have adjusted her dosage slightly and on her nurse practitioner’s recommendation we have adjusted the timing of a med that is intended to help her sleep. She takes that about thirty minutes before she heads to bed.
These slight adaptations seem to be working for her, not always but for the most part. She seems to be sleeping better and generally through the night except for the occasional bathroom trip. In addition she occasionally makes the bed – well twice so far – because I think she feels good enough (rested enough) to do that little chore.
After the second time I thanked her for making the bed up and got push back in the form of, I know how to do it!
AHA – store the little victories away in your heart for later. Keep your mouth shut if you are unable to make your praise and thanks not sound demeaning. And do not take it personable when she snaps at you, for at that moment she is there as she always was before this disease of Parkinson.
And never raise your volume, she will think you to be angry whether you are or not.
Every morning at 7AM the extremely LOUD, BRIGHT AND ANNOYING alarm clock sounds its happy tune to remind us that it is time for Cheryl’s first dose of various meds. My job is to get up and find them. I get a glass of water and bring them back to the bathroom. All of this disturbance usually awakens Cheryl. I help her get up and shuffle into the bathroom to the toilet and then to the counter to take her meds.
Her fingers may not be working well in the right-after-get-up time. At 7AM and a little, she dropped one on the floor. I got her to take the rest of her meds and eased her back to bed. I laid down too after finding that the little white pill she dropped was to combat her orthostatic hypotension which is low blood pressure associated with Parkinson disease. I put this pill with her vitamins that she took later while eating breakfast.
She takes midodrine to combat the hypotension. Generally it seems to work. This morning when she took it separate from her other meds but with her vitamins and shredded wheat, she became lightheaded and fainty feeling. When one checks out the link I have provided, one finds a wearying array of side effects, all of which or none of which are associated with other meds that she takes.
This morning she fainted while I was talking to her. She was looking gray in the face at the time. I helped her to the floor and propped her legs up on a chair. I sat on the floor with her for a bit until she felt like she could sit up. I outweigh Cheryl by about a hundred pounds or so and to me she feels pretty light. I also forget that we are the same age and that means neither of use is twenty-two anymore. Nevertheless I help her up by positioning a chair nearby and she pulls herself up or I get behind her and lift her straight up with my legs. I probably should not lift her but she really does not weigh much in my mind.
While writing about these little happenstances in our life with PD I run across a world of information about what to do and who to call. This website (https://seniorsafetyadvice.com/about-us-2/) is a wealth of information.
It has been awhile since Cheryl fainted while eating breakfast. A couple years ago it was sort of common and occurred maybe once every other week or so. It was so commonplace that I staged a pillow from our couch in one of the kitchen chairs to put under her head for a bit while she was laying on the kitchen floor recovering. Thinking back on it, it crept into our lives so gradually that the two old people living this Parkinson life thought little of it other than, oh crap another new thing to deal with.
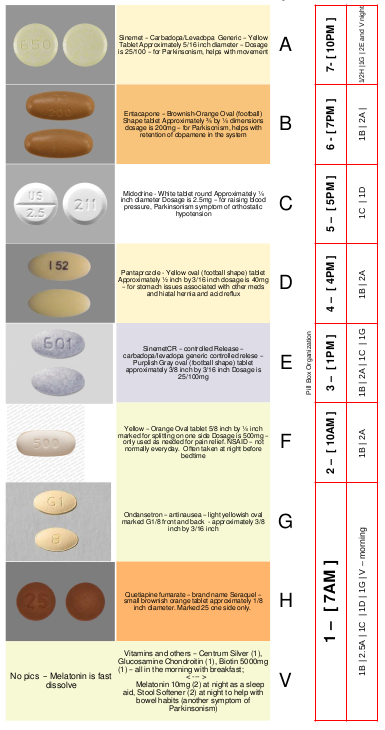
A casual mention in conversation to the medical team in a visit a couple years ago caused Maureen to give me the “stink” eye look which said to me, when were you going to mention this? I realized fainting is not a good thing or even a thing that we should merely deal with over time. She gave Cheryl a prescription for midodrine and instructions to take two when you get up and two more during the day spread out. Later this was adjusted to one in the morning, one mid-day, one no later than three hours before bedtime. I now had a use for all seven boxes of our meds organizer.
I found this a couple years ago on Amazon. Ours has black lettering and I created a chart to stick inside the lid.
A pretty long story but in addition to this little blog of mine I have started a little log of anomalous activities and the surrounding circumstances. The doctors and nurses are not looking at Cheryl every day. That is on me.
It was a miserable eve. Cheryl has had her meds adjusted a bit to help with creeping dementia issues. The doctor has been slowly increasing the dosage to creep up on the optimal dose. The most common side effect is nausea and vomiting. The new prescription is at the optimal dose and it appears Cheryl cannot tolerate it at that level. She has been sitting on the bathroom floor on and off for most of the afternoon.
As she was building up to this dose for the past several months, I expected to see some behavioral changes. I have not. As the situation got worse I terminated giving this med to Cheryl.
But last night (New Year + 1) was very difficult and very different. I thought that perhaps this drug did not work for her but it did reduce and eliminate the strange compulsive behavior that she exhibits. She also became delusional. She was certain I did not belong here.
On the next day, Monday, I called the doctor’s office and got her nurse practitioner on the phone. It is hard to explain how excited I was to have someone call back that knows Cheryl and her condition and has seen her on a regular basis. I explained what Cheryl was going thru and that I had discontinued the medication to relieve the symptoms. The NP recommended that I adjust one of the meds she was already taking with no ill physical effects and perhaps Cheryl would sleep solidly through the night and do better the next day. It worked.
Still searching for clues at the scene of the crime (Joe Walsh).
It’s a new day. Today is football day. Seems like everyone everywhere is tuned to some kind of football game. It used to be, many years ago, a time to visit our in-laws. Our niece’s birthday was January 1st. She died a year or so back not from the Covid dilemma but from other health issues. She had not been well for some time. We have not celebrated her birthday for some time. Families are complicated and estrangement is often part of the complication.
It’s a new month. January is often cold but it seems to take winter some time to get started. This January is no different. It is rainy and poopy outside today and the temperature is expected to drop into the upper teens overnight. I am so glad we live in the times we live in. It will not be necessary for me to add coal to the fire for overnight nor will it be necessary for me to huddle underneath a buffalo skin.
The current federal administration authored a congressional bill referred to as “build back better”. The previous administration had a motto of “make america great again”. Both of these are ludicrous. Both imply that there is something not quite right with now. That is absurd. Nothing is wrong with now. We are not heating with coal or huddling under buffalo skins. Slowly, ever so slowly we are converting to electric powered transportation.
Now is not perfect, of course, but it is greatly better than what was. We often think what was is better that what is. Still searching for it, clues, that is. Try to enjoy and be in the moment.
It’s a new year and thank God for that.
Resolutions? Yep. Do better at living now not ago. Try to not get fat living now.
This is Parkinson’s Awareness month but for me it is just another month. I have expanded these thoughts and comments specific to Cheryl. In the comments below I have added information that she might say but these days Parkinson’s has robbed her of language. She can speak fine but words can be hard to retrieve and occasionally some severe confusion about what is coming, where she is, or, for that matter, what happened moments ago.
Nevertheless
To the Ones That Love Me…This is what you need to know about me and my Parkinson’s Disease.
This is not a death sentence, PD can be managed. Encourage me to exercise daily, it is MY MEDICINE. – It is remarkable how much a few simple exercises can help Cheryl. Many of the exercises are simply vigorous movements or stretches. At her Parkinson Community Fitness the class exercises are tailored to folks dealing with PD. She cannot do all of the motions that the instructor asks but she tries her best to do them. The exercises can pick her up in a way that acts on her body like an extra dose of meds. Many times afterward we will have a late lunch somewhere because she is feeling good.
Early on she recognized how much exercise helped her to feel good. When her mom was still alive she spent a great deal of time at Bridgeway Pointe helping Elaine with various things. Elaine regularly exercised on a recumbent bicycle-like exercise machine. Cheryl did this as well with her mom and occasionally with me at the YMCA. She sought out an exercise regimen at the Y with one of the trainers there and developed some exercises specific to her particular inabilities. Later when PCF opened we joined. It has been and still is perfect for a non-athletic person such as Cheryl.
Don’t make assumptions about my PD, every case is different. – For many years Parkinson’s symptoms for Cheryl were mainly physical. This is no longer true. Hallucinations, delusions, mental confusion and memory loss have added to the morass of physical symptoms.
A meditation – serenity and peace comes to me when I can see that Cheryl is safe and unafraid. Most things that occur with PD cannot be changed. It is very hard to accept that fact. It is a degenerative disease. In my manliness I can see, or think I can see, ways to mitigate and ease her mind, life, anxiety and worries. And when I have done that I have removed any small bit of independence that she still has. In Cheryl’s mind oft times her disability does not exist. She has yet to capitulate. A confused mind does not recognize its confusion.
My meds have to be taken EXACTLY on time everyday. Spontaneity is no longer, please help me plan ahead. — This is complicated by the fact that what is eaten either before or after greatly affects the usefulness of the medication. The primary treatment of PD is a combination of carbidopa and levodopa often referred to as Sinemet. PD is a result generally of a dopamine deficiency. Absorption of this chemical occurs in the gut and the presence of other proteins inhibits absorption. So, “Hey. I’m hungry let’s go grab a burger somewhere!” spontaneity is gone from our lives and has been for some time. We often forget that and opt for spontaneity anyway.
That being said, Cheryl greatly enjoys the company of others (friends, siblings, past acquaintances) during dinner or lunch and she easily loses track of time and pills, food and drink get out of sequence. Her body’s reaction to this is twofold; she becomes exhausted (but not always) and she may develop severe indigestion (but not always). She may have either, none or both reactions.
My health comes first. I need to put myself before other’s needs and responsibilities. – but Cheryl is unable to do that easily. it is not part of her personality. It never has been. She is the oldest of six children and as they were growing up, her mom gave her more and more things to do and help with. I tell her often that what we do and where we go is really up to how she feels. She knows that she needs to put herself first but she would rather be with family and friends even when she is feeling not so good.
The other aspect of this is that she may feel perfectly fine until we are somewhere for a bit and she will crash. After she recovers she will become apologetic and worry that she has ruined everyone’s experience.
Anxiety is real. Don’t overwhelm or over plan me. – I have over time gone behind Cheryl’s back, so to speak, and have suggested to organizations that Cheryl is involved it that they find another to perform whatever little task she has been doing for them. She was the go-to person for anything computer related. It was her career for many years. These days it is merely a source of anxiety and confusion for her. It has reduced her anxiety level and in some cases has made me the bad guy.
I am okay with being the bad guy if she sleeps better at night.
Sometimes l am exhausted, especially late afternoon and evening. – This happens most often after she has taken her medication. It seems the meds can overwhelm her body but not always. “Always” would be easier to plan for.
How I feel changes by the hour. I can feel good in the morning and terrible an hour later. I am not the old me who can multitask and go-go-go… – It seems that any sort of multitasking activity is gone from Cheryl’s life. I however like to whine about how many new things I take care of in our life now. Cheryl no longer drives. I am her driver (whiny voice).
Be patient and don’t overwhelm me. – two questions in a row overwhelm. If that happens with me nearby, I will answer for her and slow the conversation so that she can keep up. This can include repetition.
Apathy is real! – And sometimes attention deficit is real also. It is easy for her to start one thing and be distracted by some other thing.
Sometimes l just can’t do a task and need your encouragement. – Like puzzles.
Communicate with me on your concerns and help strategize new ways of doing things. – This is a constant activity in our house. It is easy to use up days thinking about and trying new ways of doing things. It has also taken some time to train the care giver (me).
Help me to eat clean foods and drink lots of water. – Cheryl really does not like vegetables of any different variety that was not fed to her as a child. I do not know if this has any truth to it but there are many things she will not eat or even try. Her idea of lots of water is two or three sips. These are my observations from my experimentation with Hello Fresh meal kits.
As a caregiver it is hard for me to explain how frustrating some of these nuances can be. Resistance of personalization of this disease is very hard to do. I mean this two ways – projecting my feelings, what I think she is feeling, onto Cheryl and dismissing what she tells me that she feels. One of the comments above is that every case is different. This is not unique to PD. Scientific medicine would like the mechanism of disease causation and progression to present as a commonality to all humankind but that simply is not so.
There is a lot of discussion of phases of Parkinson’s disease in medical texts and websites. From my narrow view that is mostly crap. Literally everyone is different. It serves no purpose to relate current symptoms to some list and determine were one is in the dance we all have with death. It is best to look for and act on the feeling good times. There will be plenty of time to consider the feeling bad times after one has passed from this life.
Almost fifteen years ago this summer is the time that I found out that I was a match to my youngest sister Laura. She had found out earlier in the year that she had Myelodysplastic syndrome. Her body was turning on her. She would die without treatment. Then our whole family was still alive.
Mom and Dad still lived in their home in Madisonville. My elder brother lived in Florida near Orlando with his wife. My younger sister Joyce lived with her spouse in Portland Oregon. Laura and her husband lived in south eastern Indiana and Cheryl and I lived in southwest Ohio in Cincinnati. Now only Joyce and I are still alive.
I think of these things when I donate blood four times each year. I ponder how long I can donate blood. The only answer I get when I search for that information is, as long as you are healthy, you can donate.
This started with Laura but I had donated blood before, just not on a regular basis. When I was in school at the University of Cincinnati in the last millennium an instructor whom many of us liked let slip some personal information about his family. His son had been in an accident and needed blood donations. Several of us went to Hoxworth to donate. I was too young so permission had to be obtained from my parent. Looking back this detail seems odd. I was eighteen at the time.
With Laura’s diagnosis and need for blood stem cells all of us siblings were tested to see if any of us were a match. Only I was a match. I found this out from the nurse who called me as was driving back towards Boston from Cape Cod. We had gone there for a little vacation and to visit with friends. This was convenient for Laura and me as neither of us had to travel far to do this but I had to get home first.
The summer of 2007 was a long one for Laura and me. I cannot speak for Laura because she did not make it out the other side of the treatment process. I am changed forever.
The process takes several days. For me it involved a very thorough physical and several meetings with the medical folks at the end of which I was deemed healthy enough physically and mentally to go through the process. During one meeting with a nurse who also had background as a sociologist, I was made aware of the fact that there was a chance that during the implantation process my stem cells could take over her bone marrow and give rise to my immune system within her body and reject her. Not simply that it might not take and we would have a do over. My immune system would reject her. Seems like a bad thing to happen, to be rejected by your own immune system.
Blood stem cells are removed from the donor in two ways either directly from your hip or by apheresis . In Laura’s case they used apheresis to remove blood stem cells from me and gave them to her after killing off her bone marrow’s ability to produce blood cells. Over a period of several days – my memory tells me four – I was given an injection of some growth hormone that told my body to make way too many blasts (precursors of various blood cells). These leak out into the peripheral circulatory system and can be retrieved by an apheresis machine. It was a miserable four days. Not so much at first but they can give you the injection anywhere and I opted for my arm. I am pretty sure that this started on a Monday so we were ready to do the apheresis on Friday. The had to get the blasts out of me before my body reabsorbed them.
The apheresis process takes a bit of time also. I do not remember talking about the actual process at the beginning. I suspect that if the donors are given all the gruesome details at the start, some will back out. The process was generally described as similar to donating blood except that the stem cells would be removed and the rest of my blood would be given back to me.
An innocuous drawing
In this sketch you can see the general set up. Blood is removed from one arm and the returned processed blood is put into the other arm. Pick your nose, pee and fart before you get started because there is no moving around once the machine is running.
I asked the nurse technician who was monitoring the machine approximately how long it might take and she responded with eight to nine hours for the first session. She said sometimes they do not get enough the first time so they have to do it again to get more stem cells. I intermediately got up to find the men’s room and empty everything out and began to worry about how long my bladder would hold out. In the end it was not a concern. I suspect my kidneys did not understand what was happening so they elected to take a break for a few hours. I helped by not drinking anything of course but there was a bag of saline as a part of the process and some blood thinners to keep my blood from gumming up the pumps. Nine hours is a long time to sit.
Making conversation I asked how many cells they were trying to harvest. Ten to eleven million came the reply. I remember thinking that seems like a lot but I did not have any idea what they might need to do this. I was curious how they would figure out how many they had and she told me they would count them. It is amusing when you think about it. how else would you figure it out. Isolate a certain quantity of serum and under a microscope count the stem cells. Well, huh. Even an engineer can do that.
With all the needles and tubes in the correct position we started. I think the first session was about seven hours or so. There was a clock, one of those battery jobs, hanging on the wall opposite where I was sitting. What a poor place for an ineffective time keeper to hang. After five hours I was certain that it had slowed down. After six hours I was certain it had started running backwards ever so slowly. At the seven hour mark the stem cell bag which I estimated could easily hold a liter had a tiny amount of yellowish life saving liquid in it. The nurse pronounced it good and Cheryl took me home.
Oddly I was incredibly tired. I had not felt this exhausted before. I had not moved all day. But my blood did. It had been in and out of my body about ten times during the day. It was wore out. As I rested in my chair hovering between resting and sleep we got a call from the hospital, I needed to come back again for a second session. How many cells I asked. About four million was the answer. A disappointingly low number, I was certain that they would need two more times. I may have said shit out loud.
On the second day the procedure the was much faster. I spent approximately four hours in the chair with the stopped clock view. Often the donor’s body wakes up and puts more cells out there where the apheresis machine can find them. But that is not really why I am telling this story. There were several times during the next couple of weeks when I was called to go directly to Hoxworth to donate other bloods products to Laura. Platelets mostly as I recall. On a couple occasions I gave Laura platelets. I may have given her red blood cells also but I am unsure of that. She was busy staying alive and I was trying to help. All of these experiences got me used to the activity of donating blood.
I started doing this at the main Hoxworth Blood center near UC Hospital in Clifton and then later discovered that I could do this at another collection center in Blue Ash, Ohio. Once when I was there donating, the nurse technician asked me if I had ever considered giving a double red. After a discussion of what was entailed and other questions, I tried it.
This is Laura’s legacy. Her brother became so comfortable with donating he continues to do it fifteen years later.
I often think about Laura when I am sitting in the chair listening to the apheresis machine do its thing. There is no stupid clock to stare at. I know now how long it takes. It takes thirty to forty minutes. Sometimes it takes longer because the technician is often monitoring other donors. Most often I read a book on my tablet reader. Occasionally I listen to the patter of conversation around me.
Hoxworth is actively soliciting folks who have had SARS CoV2 disease because their blood contains substances that can help those who are recovering from that disease. These folks sit across from where I am donating.
Over the weekend the reward for donating was a free T-shirt. Free t-shirts were the give away today, Easter Monday also. I selected a St. Patrick’s Day themed shirt. It is in the picture.
Laura’s recovery was long and arduous and fraught with disaster. She spent about six weeks in a coma as doctors tried to discover the source of her liver inflammation. Veno-Occlusive disease was the suspected culprit.
Hepatic Veno-Occlusive Disease (VOD) AKA: Sinusoidal Obstruction Syndrome is a well recognized complication and leading cause of mortality in hematopoietic stem cell transplant resulting from severe hepatocellular necrosis and hepatic vascular congestion. — This is from a medical teaching website. Laura and I both read about it in a big white binder that she had gotten at the beginning of her process. I remember her looking at me that first afternoon with her yellowish face telling me that there was about a 3% recovery rate. Pretty crappy odds she said. She was a CPA and the controller of a small successful beverage distributor. She knew about numbers analysis and crappy odds.
It was not that. Eventually the doctors discovered that Laura was having a bad reaction to the antibiotics given to her as a prophylactic to infection while my stem cells were taking over. She did recover but six weeks asleep devastated her body. During a visit at the holidays she told me that my stem cells had populated her bone marrow and was doing fine. A few weeks later she succumbed to pneumonia that could not be treated in the conventional way because of her problems with antibiotics.
Laura died with a part of me in her. Part of me died when she passed out of existence in early 2008. Watching someone whom you worked so hard to save take their last breath is a profoundly life altering experience. I hope to never participate in an experience like that again.